Category Archives: Hospital life
Donate to Keep Abortion Access Available in the West!
Around the same time as Margaret Sanger was going door to door through New York city, another young woman was faced with an unintended pregnancy. Already having two sons, there was no way her family could afford another mouth to feed. My great-great grandmother attempted a home abortion and died.
I love working for Planned Parenthood. Every day I am able to help young people access birth control safely and plan their fertility in a way that will allow them to be young people. I help mothers who were told breast feeding was enough. I help 45 year old women who thought they were “done with all that” (FYI – you’re not). I help trans folks and LGBTQIA folks and I am able to help so many people through my work at Planned Parenthood.
If you are getting this email, you’ve asked me for favors or money or some kind of help in the past, and I hope I was able to provide it. Right now, Planned Parenthood needs you. We need to be able to continue the valuable and lifesaving work we have been doing this entire time.
Please consider making even the smallest of donations. A couple dollars pays for a handful of condoms that we can pass out to 10 different patients. Planned Parenthood is an incredibly frugal organization. We quarter our sticky notes. We push ever single dollar as far as it will go. Please know that a dollar given to Planned Parenthood is a dollar that will help many people, many faces, faces that look like people you love.
With my nurse’s stethoscope (inspired by @lilredrooster)
I have:
Heard a collapsed lung.
Informed the doc my patient had symptoms of a pulmonary embolism, NOT pneumonia.
Heard fluid and asked for a chest xray to confirm pneumonia
Heard new onset afib before the EKG could get in the room.
Heard that terrible sound a heart makes when there is an incredibly high potassium level
Listened to bruits and thrills.
Heard crackles, rales, wheezes.. and that awful silence.
Confirmed the nasogastric tube I just placed was in the correct spot.
Recognized anaphylaxis and called the code, enabling anesthesia to get there in time
Listened to the racing hearts of newborns
Listened to the last beat of a woman’s heart as I held her hand, like I promised I would.
Caught a BP too low for a machine to catch.
With my nurse’s stethoscope I have saved lives.
I have never borrowed a doctor’s stethoscope because if I ever didn’t have my own, another NURSE lent me theirs.
Change the narrative. Learn what nurses DO.
“Sexy” Nurse Costumes Harm Nurses
It’s Halloween, the time when people seem to lose their respect for others and find the most offensive costumes ever. It’s this time of year when my Facebook feed, Twitter TL and email fill with ads people think I should see.
Here we go.
Ebola nurse.
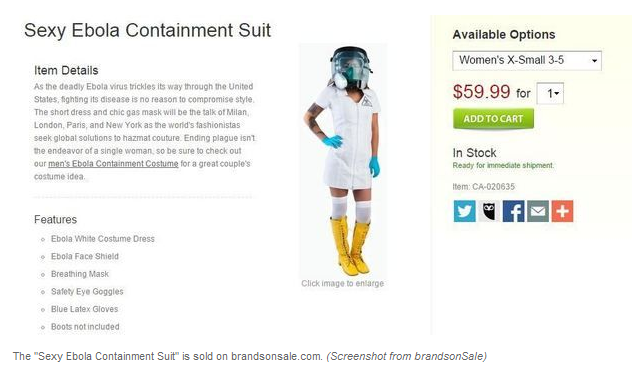
While another photo circling the internet was photoshopped, the above photo was not.
Let’s remember that hundreds of nurses have died from treating Ebola patients in West Africa. Not because they are lazy or sloppy but because the number of patients and lack of protective gear means nurses have a very high chance of disease. Recently, several nurses died of Ebola after caring for a newborn who had the disease. Their choice was to pick up the baby and care for it or leave it in a box to die.
It’s a long shot, but I believe the “Ebola nurse” costume may be the most offensive Sexy Nurse costume of them all. Already I know some person with very poor judgement and a large amount of racism is going to combine a sexy nurse costume with Blackface and call themselves Amber Vinson. That will be the most offensive I have ever seen. If you see it, don’t tell me about it. I don’t want to know.
(Anyone who puts on Blackface, Yellowface, Redface for costumes is out of line. It’s racist and harmful. Period. Don’t do it. Google “should I wear Blackface” and see what you find out)
I am THRILLED that Amber Vinson, RN and Nina Pham, RN have been cured of Ebola. I am THRILLED. They contracted Ebola in the service of their patient and they deserved the best care the US had to offer and I am so glad they got it. I am also glad that there have been no further cases (as of now) out of Texas.
But what the hell are you doing dressing up in a sexy “Ebola nurse” costume when there are nurses in West Africa probably dying of Ebola right now?
About 2 months ago, I received an email from the CDC, asking for volunteers to train and go to West Africa for 4 week periods of time. I did not answer it. I spent most of the Spring season ill with pneumonia and pericarditis. I am not in the kind of shape to go to West Africa and work 24 hour shifts caring for Ebola patients.
But other people did. Right now, Kaci Hickcox, RN, is sitting in a tent in New Jersey, in paper scrubs. New York and New Jersey say this is their plan for healthcare workers who return from treating Ebola patients in West Africa. Humiliating treatment for a person who has spent a month caring for the very sickest of patients, who watched a child die of Ebola her last night in West Africa. This is a person who has risked her life. She deserves better than this.
Sexy nurse costumes are not funny. Don’t wear a sexy nurse costume. They’re disgusting. If you want to be a nurse for Halloween, wear real scrubs. Being a nurse is an honorable profession. and not worthy of being mocked or sexualized.
In the blog post that made my life miserable, “The Effects of Nursing on Nurses,” I talked about the heavy mental and emotional toll nursing can place on a person. That was a post made after three incredibly busy night shifts when I was tired and dismayed at seeing a nurse I admire burst into tears. I’ve had some pressure to take the post down, but I’m going to let it stand because it still gets about 50 views a day. If any of those views are a nurse looking for someone who feels the same way, the post should stand.
Sexy nurse costumes add to the burden nurses already bear.
Nurses are highly trained professionals who put themselves at risk for you and your families over and over again. In my career, I have been groped, hit in the abdomen, smacked in the face, and smacked on my behind. I’ve had a physician slide his hand up my thigh. I’ve been called a bitch and a cunt, by PHYSICIANS. In addition to these physical assaults myself and nurses everywhere are frequently subjected to harassing comments, jokes, and behavior. This IS workplace sexual harassment, and somewhere right now, another nurse is dealing with it. Nurses are expected to laugh off harassing behavior and very few patients ever experience repercussions.
Nurses who are attacked by patients or even physicians rarely are able to seek justice for themselves. I do not know of any cases where a patient has been successfully prosecuted for sexual harassment of a nurses. This is similar to the behavior experienced by waitstaff. Additional cases of nurses who have tried to take on physicians can be found in Suzanne Gordon’s Nursing Against the Odds. I also Tweeted extensively about laws in Texas that do not allow for anonymous complaints against physicians and hospitals. For more information, you can check the #WinklerRNs hashtag, which stands as a reminder to what happens to nurses who whistleblow in Texas.
And last, I’m going to talk about costumes for doctors and costumes for nurses. See below:

Here is another advertisement, this time showing 9 nurse costumes and one doctor costume. Notice the difference? The doctor costume is not hyper-sexualized, it’s respectable. This advertisement is a symbol of how nurses are perceived by the public. When you wear a costume like this, you degrade nurses. If you look back in your life, or talk to your parents, you know nurses. You know someone who works long hours, through the night, and you probably have a story of how a nurse saved someone’s life.
I was wearing a blue plaid shirt and jeans the day I stopped on I-25 near the Colorado/New Mexico border to aid a man who had hit the side of a mountain. He had been flung from his vehicle. As I ran from the South side of the interstate to the North, I saw at least 20 people standing around him. I asked for help, and no one responded.
I quickly assessed the man and noted he had multiple broken ribs, resulting in a flail chest, which compromises breathing. He had a head wound, compound fracture of the leg, and an arterial bleed from his arm. Someone had thrown a towel over him.
I knelt over this man, clamped the towel around the artery, put pressure on his ribcage with my knees and secured his airway. Immediately, he drew in a breath, his color returned and he began to struggle. Still, none of the bystanders would come to my assistance. I was stuck. I was using every piece of my body and strength to hold this man still.
After what seemed like an eternity, the paramedics arrived, listened to my report and took my place. I got back to the car and cleaned up with the bleach wipes I keep there.
Do I deserve to have my image and profession mocked?
That’s what a nurse looks like. Someone risking their life for yours. Don’t degrade us. Don’t mock us with hyper-sexualized costumes. Respect nurses. As someone said on my Twitter timeline last night, “we are here to save your ass, not fuck it.”
Edit: Prior to writing this post, I had not seen any “sexy male nurse” costumes, so I did not include them. I was wrong.

Concerns and Suggestions About the Future of the ADN and the BSN
I am finishing my BSN, FINALLY, and I have …. concerns
When you view the chart, realize that the higher in the chart you are, the fewer years of experience you are actually receiving.
Above is a link to a rough post where I have graphed a very rough flowchart of where I think nursing is heading. I believe current goals will result in a forced exodus of experienced nurses from existing acute care facilities when they are not able to accommodate their schedules and finances to higher education.
I believe the push for higher nursing education is a good one, but if hospitals want to keep their best nurses, they need to begin to formulate a plan that sets aside paid time for educational goals and work with universities to bring the needed education into the hospital. BSN programs need to be closely reviewed to be sure the information they are teaching ADNs is relevant to practice and the goal should be to increase knowledge of the ADNs instead of simply fulfilling the core tenants of a Bachelor’s degree. In a utopic situation, the course would be created so that ADNs coming into a BSN program would actually emerge with a certification reflective of their years of experience and knowledge and placing them higher in the nursing hierarchy than new graduate BSNs with no experience.
Yes. This will require hospitals to pay nurses floor pay to attend classes. The hospitals will benefit with higher patient satisfaction scores, lower patient injuries, and better physician/nurse relations. Many hospitals already offer education assistance and scholarships in exchange for time worked after graduation. This does not need to be any different.
If nurses have time set aside for classes that they are attending with their coworkers, they have a ready made support system, which is necessary for successful education. If nurses are allowed to work fewer hours on the floor while they are receiving their education, advancing ones education will not appear so monumental and burdensome.
As far as funding these paid hours that are performed off the floor, hospitals should look to their political force. This is a viable method that can be used to increase the knowledge and the size of the nursing force, at a time when an influx of patients threatens to cripple the current United States medical system. Nurses will emerge from these programs empowered, better team players, and will receive knowledge they can apply to the bedside at their next shift rather than trying to find time to take off work, struggling through APA format and trying to find a way to pay for their own college education as well as that of their children.
No ADN currently working full time should be forced to carry a burden of student loans to maintain their current career. This is a burden that many nurses with families and current student loan debt cannot handle. Instead of requiring 2 years of work in order to receive student loan relief, while paying student loans, give the relief IMMEDIATELY, and require nurses to pay back a prorated sum if they leave the area or change careers.
It is my belief that this kind of incentive is what is needed to get ADN nurses into BSN classes. Current BSN programs focus on papers and theory, but there is very little meat added to the pot of nursing experience already held. This is a waste of the time of experienced nurses. Because it has already been decided that management roles should be held by holders of nursing doctorates and master’s degrees, only individuals who are interested should be required to take additional classes in nurse management. Nursing programs need to be divided into tracks: Research. Management. Advanced Care. Hospital Management.
Instead of this, we have nurses sitting in History, Music and Philosophy classes to earn their BSN. All of these are valid courses of study but are they actually efficient for people whose priority is to get back on the floor? Nurses who have an ADN and have years of floor experience do not necessarily need these classes but could use classes in new techniques, evidence based practice, and advanced practice.
As a floor nurse who has worked in multiple hospitals, including LTAC, rehab and nursing homes as I made my way up from being a tech to a RN, I feel the the nursing profession is missing a valuable opportunity to increase the abilities of their current workforce while making nursing a more rewarding experience.
What About the: Respiratory Therapists?
Ready for a happy story?
Respiratory therapists are responsible for a lot of things all over the hospital. When they are on our floor, I can hear their phones ringing to call them to another floor. We see them doing treatments frequently, we call for help occasionally, and they are always included in a rapid response (a team effort to get to a deteriorating patient and avoid a code).
I am good with trachs, due to extensive training while I was a tech, and later homecare experience. So I am very comfortable with suctioning and trach care. Often, if the RT is very busy, I’ll do as much as possible to make their night smoother. I also volunteer to take the trach patients as often as I can because I know most of the nurses on my floor don’t like trachs. These patients often request for me to be their nurse again and again, and I do. It helps that I’m an excellent lip readers and intuitive. I rarely feel fear with a trach.. it’s a stable airway.
Recently at work, I felt helpless. It was a busy night, I had a 6 patient load with some really heavy patients. My patient was deteriorating and a call to the resident was fruitless. I suctioned, but it was like tar. It was bad. My patient was grey. The oxygen level was okay so far but could get worse at any moment.
For the next 1-1 1/2 hours, two incredibly knowledgeable RTs worked over my patient, performing procedures I’d never even heard of. They told me what medications to get from the doctor. I phoned and phoned and phoned. I brought the meds in. I medicated the patient for pain. Other respiratory therapists in the hospital started to pick up their work, but I know they got behind.
It’s the middle of the night in the hospital. We ran out of suction catheters. The house supervisor went to central supply and when she couldn’t find what we needed, so she called floor after floor and suction catheters start to appear. We were good.
I was so impressed by the variety of the things they could do, and within that hour to hour and a half, my patient began to breath better. Partially from pain medication, but mostly from sheer force of will. We are all very bonded to this patient and he to us.
I was also impressed by the nurses and CNAs who left their floors running with the equipment we so desperately needed.
When I left that morning, the patient put out a hand. Thanked me for all I did. I said
You’re welcome, but it was a team effort and you are the most valuable player in the team.”
A lot of times, you’ll have a bad shift and you’ll feel you didn’t give the best care, and you’ll say to the oncoming nurse “well, they’re all breathing.” It’s nurse code for “I could only do the bare minimum, but we all survived, can I go home now please?
That night, I learned more about what respiratory therapists do. Like nurses, they run hard, unlike nurses, they are spread throughout the hospital covering several floors at a time. I knew they were smart, good in a crisis, but I am so moved by gratitude.
When I left work, everyone was breathing. And that is because the respiratory therapists I work with put their feet down and said “no.” It was a rough night, but we gave excellent care. And honestly, I don’t begrudge that patient my break (I did manage to eat). In a perfect world, nurses could get breaks everyday but medicine is by its own nature an imperfect science, and while I complain if I don’t consistently get breaks, it is absolutely worth missing a break to improve your patient’s health.
I plan on writing a series of blog entries about my interactions with other medical professionals. As with my patients, I will not name names or identifying features. The only person’s privacy I am giving up is my own.
