Blog Archives
With my nurse’s stethoscope (inspired by @lilredrooster)
I have:
Heard a collapsed lung.
Informed the doc my patient had symptoms of a pulmonary embolism, NOT pneumonia.
Heard fluid and asked for a chest xray to confirm pneumonia
Heard new onset afib before the EKG could get in the room.
Heard that terrible sound a heart makes when there is an incredibly high potassium level
Listened to bruits and thrills.
Heard crackles, rales, wheezes.. and that awful silence.
Confirmed the nasogastric tube I just placed was in the correct spot.
Recognized anaphylaxis and called the code, enabling anesthesia to get there in time
Listened to the racing hearts of newborns
Listened to the last beat of a woman’s heart as I held her hand, like I promised I would.
Caught a BP too low for a machine to catch.
With my nurse’s stethoscope I have saved lives.
I have never borrowed a doctor’s stethoscope because if I ever didn’t have my own, another NURSE lent me theirs.
Change the narrative. Learn what nurses DO.
CIrcle of Love for Mama Josie

Josie Shapiro is one of the threads that holds Denver’s eclectic bunch of activists together. Whether it’s raising funds for a funeral, for bail, or organizing a march to proclaim that Black Lives Matter, Mama Josie is always there to Defend Denver.
Last year, Josie and her then partner Dave donated their entire savings to pay for the funeral of Ryan Ronquillo, a young man murdered by Denver’s gang unit. After the funeral, they worked tirelessly to organize marches and keep Ryan’s name in the news so that his death would not be forgotten.
After making her activism so visible to the community, Josie found herself tailed by police. Because of her activism on behalf of the Ronquillos, she lost her job, which she dearly loved, providing doula services to families on their journeys to becoming parents.
Not only did Josie donate her own home to use to raise funds for the Ronquillos, she also raised money for the family of Jessie Hernandez, who was killed by the Denver police in January. Like most of the Denver activist community, she found herself mourning the loss of a vibrant teen while also fighting for the freedom of Sharod Kindell.
At a meeting of activists several months ago, the mother and father of Jessie Hernandez expressed, through tears, their love and appreciate for Josie and the tireless work she had done to help them pay the rent, buy food, and bury their child.
Now, Josie finds herself alone. She and her partner of 6 years, the father of her children, are divorcing. Josie is about to find herself without a job, without a car, without a partner, and if we cannot help her through this, without a home. She is looking hard to find work, but continues to pay a heavy price for her activism.
There is no way this amazing, dedicated young woman should lose her home and her independence when she has done so much for her community. Please help us by joining the Circle of Love for Mama Josie, and donating what you can today. Every dollar helps a woman journeying into single motherhood provide for her children and stay in her home.
If you cannot donate, please help by sharing this post on Facebook, Twitter, WordPress, and other social media. Donations of social media platforms are absolutely donations!
Thank you.
Shiftwork and Activism
From my Facebook Page:
I am going to make a request. While i have tried to be very vocal about this, and the majority of people are respectful, I need to make it clear:
I am a night shift nurse. This means I only work 2-3 days a week and occasionally have meetings at my hospital. This allows for a lot of time to organize and to go to meetings.
What it does not mean is that I can skip sleep to go to meetings. I cannot sleep for a few hours, then go to a meeting, and then go back to sleep. I cannot exist on less than 7 hours of sleep. It is not safe for me. It is not good for my patients. It is also not good for organizing because there is a big chance I will forget what we have been talking about if I have been up for 24 hours.
I work at least 2 weekends a month. I do not have a set schedule, and my work is scheduled 2-3 months in advance. Yes, this can be inconvenient. No, it is not unfair. Most nurses work at least every other weekend and many holidays. Many other careers have unpredictable hours. This should not exclude us.
A Monday through Friday, 8-5 job, is a privilege. It affords you opportunities shift workers do not have. When people ask that meetings be scheduled at more inclusive times, or if multiple meetings can be scheduled around one topic, this is an opportunity for inclusivity.
I love my job. I love organizing. I can do both.
As I have gotten more involved with activism online and out in the world, I have tried to make myself very accessible and available. It is time to set some limits. I will check phones messages, emails, tweets, Facebook updates, etc frequently if I am not asleep, at work, or driving. If I am doing those things, I will check in during my break, before I go to bed, and after I get up. I will no longer receive alerts for Twitter DMs on a regular basis. This is for my mental and physical health.
I know a lot of other shift workers feel this way. I would really appreciate if you are a shift worker and you have trouble with people respecting basic needs, that you post here and talk about it.
“Sexy” Nurse Costumes Harm Nurses
It’s Halloween, the time when people seem to lose their respect for others and find the most offensive costumes ever. It’s this time of year when my Facebook feed, Twitter TL and email fill with ads people think I should see.
Here we go.
Ebola nurse.
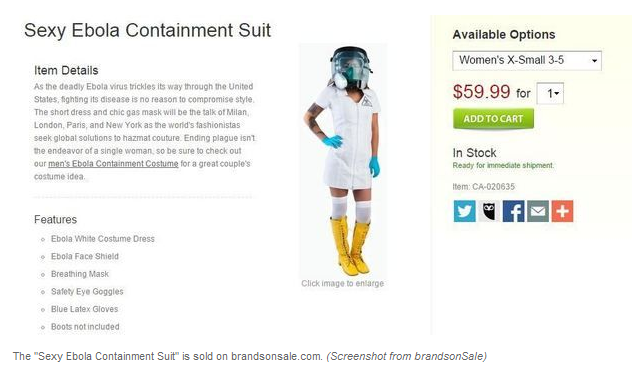
While another photo circling the internet was photoshopped, the above photo was not.
Let’s remember that hundreds of nurses have died from treating Ebola patients in West Africa. Not because they are lazy or sloppy but because the number of patients and lack of protective gear means nurses have a very high chance of disease. Recently, several nurses died of Ebola after caring for a newborn who had the disease. Their choice was to pick up the baby and care for it or leave it in a box to die.
It’s a long shot, but I believe the “Ebola nurse” costume may be the most offensive Sexy Nurse costume of them all. Already I know some person with very poor judgement and a large amount of racism is going to combine a sexy nurse costume with Blackface and call themselves Amber Vinson. That will be the most offensive I have ever seen. If you see it, don’t tell me about it. I don’t want to know.
(Anyone who puts on Blackface, Yellowface, Redface for costumes is out of line. It’s racist and harmful. Period. Don’t do it. Google “should I wear Blackface” and see what you find out)
I am THRILLED that Amber Vinson, RN and Nina Pham, RN have been cured of Ebola. I am THRILLED. They contracted Ebola in the service of their patient and they deserved the best care the US had to offer and I am so glad they got it. I am also glad that there have been no further cases (as of now) out of Texas.
But what the hell are you doing dressing up in a sexy “Ebola nurse” costume when there are nurses in West Africa probably dying of Ebola right now?
About 2 months ago, I received an email from the CDC, asking for volunteers to train and go to West Africa for 4 week periods of time. I did not answer it. I spent most of the Spring season ill with pneumonia and pericarditis. I am not in the kind of shape to go to West Africa and work 24 hour shifts caring for Ebola patients.
But other people did. Right now, Kaci Hickcox, RN, is sitting in a tent in New Jersey, in paper scrubs. New York and New Jersey say this is their plan for healthcare workers who return from treating Ebola patients in West Africa. Humiliating treatment for a person who has spent a month caring for the very sickest of patients, who watched a child die of Ebola her last night in West Africa. This is a person who has risked her life. She deserves better than this.
Sexy nurse costumes are not funny. Don’t wear a sexy nurse costume. They’re disgusting. If you want to be a nurse for Halloween, wear real scrubs. Being a nurse is an honorable profession. and not worthy of being mocked or sexualized.
In the blog post that made my life miserable, “The Effects of Nursing on Nurses,” I talked about the heavy mental and emotional toll nursing can place on a person. That was a post made after three incredibly busy night shifts when I was tired and dismayed at seeing a nurse I admire burst into tears. I’ve had some pressure to take the post down, but I’m going to let it stand because it still gets about 50 views a day. If any of those views are a nurse looking for someone who feels the same way, the post should stand.
Sexy nurse costumes add to the burden nurses already bear.
Nurses are highly trained professionals who put themselves at risk for you and your families over and over again. In my career, I have been groped, hit in the abdomen, smacked in the face, and smacked on my behind. I’ve had a physician slide his hand up my thigh. I’ve been called a bitch and a cunt, by PHYSICIANS. In addition to these physical assaults myself and nurses everywhere are frequently subjected to harassing comments, jokes, and behavior. This IS workplace sexual harassment, and somewhere right now, another nurse is dealing with it. Nurses are expected to laugh off harassing behavior and very few patients ever experience repercussions.
Nurses who are attacked by patients or even physicians rarely are able to seek justice for themselves. I do not know of any cases where a patient has been successfully prosecuted for sexual harassment of a nurses. This is similar to the behavior experienced by waitstaff. Additional cases of nurses who have tried to take on physicians can be found in Suzanne Gordon’s Nursing Against the Odds. I also Tweeted extensively about laws in Texas that do not allow for anonymous complaints against physicians and hospitals. For more information, you can check the #WinklerRNs hashtag, which stands as a reminder to what happens to nurses who whistleblow in Texas.
And last, I’m going to talk about costumes for doctors and costumes for nurses. See below:

Here is another advertisement, this time showing 9 nurse costumes and one doctor costume. Notice the difference? The doctor costume is not hyper-sexualized, it’s respectable. This advertisement is a symbol of how nurses are perceived by the public. When you wear a costume like this, you degrade nurses. If you look back in your life, or talk to your parents, you know nurses. You know someone who works long hours, through the night, and you probably have a story of how a nurse saved someone’s life.
I was wearing a blue plaid shirt and jeans the day I stopped on I-25 near the Colorado/New Mexico border to aid a man who had hit the side of a mountain. He had been flung from his vehicle. As I ran from the South side of the interstate to the North, I saw at least 20 people standing around him. I asked for help, and no one responded.
I quickly assessed the man and noted he had multiple broken ribs, resulting in a flail chest, which compromises breathing. He had a head wound, compound fracture of the leg, and an arterial bleed from his arm. Someone had thrown a towel over him.
I knelt over this man, clamped the towel around the artery, put pressure on his ribcage with my knees and secured his airway. Immediately, he drew in a breath, his color returned and he began to struggle. Still, none of the bystanders would come to my assistance. I was stuck. I was using every piece of my body and strength to hold this man still.
After what seemed like an eternity, the paramedics arrived, listened to my report and took my place. I got back to the car and cleaned up with the bleach wipes I keep there.
Do I deserve to have my image and profession mocked?
That’s what a nurse looks like. Someone risking their life for yours. Don’t degrade us. Don’t mock us with hyper-sexualized costumes. Respect nurses. As someone said on my Twitter timeline last night, “we are here to save your ass, not fuck it.”
Edit: Prior to writing this post, I had not seen any “sexy male nurse” costumes, so I did not include them. I was wrong.

Why We Shouldn’t Be Surprised a Nurse Contracted Ebola in the U.S.

Note: I have intentionally not linked to NBC’s post about Nina Pham, RN’s nursing experience. Critical care nurses must meet exacting requirements prior to receiving critical care certification. Critical Care certified nurses have already put in the time. Please reference this FAQ from the American Association of Critical Care Nurses
Anyone making comments about the nurse who contracted Ebola and her competence or her thoroughness needs to read this article. If you are a nurse or physician or other healthcare provider who does not work in a biohazard containment facility, you need to rethink. Remember: people who are experts with this clothing get Ebola. Are we surprised that people who are not experts could contract it? The issue is training and skill level. We should not be surprised that people who have never been around Ebola are not experts at containing or contracting Ebola.
(update added at end of post)
I’ve known for years (and I think a lot of people have) that Ebola would get to the U.S, but I still haven’t been afraid of it because you remain more at risk of being shot by a police officer or security guard even if unarmed in the United State than of catching Ebola. Even as a nurse. You are at higher risk to die of diabetes, the flu, or by a drunk driver than you are from Ebola. You have this risk simply because you live in the United States.
But what I DO know… due to my burn scar, I can’t wear a traditional TB mask. I have to wear a PAPR hood. However, I’ve never worn one. I don’t even know how they work. Still, if I had a TB patient, I’d be expected to learn how to care for the hood as well as the patient. I’ve never worn one. That’s…. not comforting. (In addition, workers at Texas Presbyterian were not given Hazmat suits until a positive Ebola test was received).
I think it’s time hospitals, nursing, and medical schools started adding biohazard PPE training to their regimens. I think the United States should fund this. I think they can do it by reversing the decision to slash the Hospital Preparedness Program from $515 million to $255 milllion in 2014 and the Public Health Emergency Preparedness Program from $900 million in 2005 to $610 million this year. (Links found from “Ebola Highlights Public Health Crisis“)
The United States has thousands of hospitals, all staffed by medical professionals who have dedicated years of their lives to careful education and preparedness for the care of any individual who may be hurt or ill. Is it too much to ask that the United States not ask for actual years off of our lives?
Edit:
After initially posting this, I came across this article from Oregon Live that states, according to records obtained by the AP, Texas Presbyterian did not place it’s staff into Hazmat suits until Duncan’s Ebola test was positive.
So:
Patient from Liberia: Check
With explosive diarrhea: Check
Vomiting: Check
High fever: Check
Hazmat suits? Let’s wait for blood results.
I really hope that article is wrong, but I don’t think it will be.
The History of Breastfeeding Among Black Women – What White Nurses Need to Know
If you are a nurse, particularly a white nurse, working in postpartum or NICU and teaching new parents how to breastfeed, it is vital that you understand the history of breastfeeding among Black women. Up until late in the last century, Black women were still employed as wet nurses for White families. This robs a Black woman’s own child of nutrition. It also explains why many Black women have a negative connotation with breastfeeding. Rather than blindly push forward with lactation education, nurses need to work to further develop cultural competence and understand why Black women may choose not to breastfeed, and why their relatives may encourage them NOT to breastfeed.
Ultimately, breastfeeding should be the choice of the individual involved, not the choice of a nurse or family members surrounding the new parent.
@FeministaJones made a series of tweets regarding the history of breastfeeding and black women, as well as the history of how Black nurses were treated in homes. It is hard to read, but necessary to learn. I storified the tweets yesterday, but am also placing them here so that I can quickly point to them.
On Black Women and Breastfeeding
In her #WomensHistoryMonth discussion, @FeministaJones discusses the history of Black women and forced breastfeeding of White children in the United States, up to modern times, pinpointing reasons for low levels of support among Black men for breastfeeding among Black women today.
-
If were going to talk about #WomensHistoryMonth, can we tell all of the stories, please?
-
 #WomensHistoryMonth Black Nannies after Civil War … http://b-womeninamericanhistory19.blogspot.com/2012/08/the-african-american-nanny-in-early.html … You’re welcome. pic.twitter.com/WRM1BP91iI
#WomensHistoryMonth Black Nannies after Civil War … http://b-womeninamericanhistory19.blogspot.com/2012/08/the-african-american-nanny-in-early.html … You’re welcome. pic.twitter.com/WRM1BP91iI -
Check out the link in that last tweet. Jarring images of the history of Black women as caretakers of White children
-
“Recent study, 54% of black mothers breast-fed their infants from birth, compared with 74% of white mothers and 80% of Hispanic mothers”
-
One has to wonder where the suffrage movement would have gone without Black nannies at home raising their children while they marched…
-
 RT @followmissbliss: @FeministaJones And for those who still don’t get it, there’s this… pic.twitter.com/qO7uSheBaW #WomensHistoryMonth
RT @followmissbliss: @FeministaJones And for those who still don’t get it, there’s this… pic.twitter.com/qO7uSheBaW #WomensHistoryMonth -
@FeministaJones breast feeding my son was a trigger 4 my grandmother. I couldn’t figure out why she was so upset but now.. that pic #tears
-
As well you should RT @thetrudz: @FeministaJones I feel…rage.
-
The only acceptable feeling when shown images like those, IMO, is rage.
-
Maybe I can spark enough rage to incite a revolution…
-
When I discussed the idea that Black women, esp in the 60s and 70s were largely anti-breastfeeding bc of being forced to nurse White babies
-
People suggested I was too militant and talking crazy but… I’m right.
-
There was, on the part of many Black women, an outright rejection of breastfeeding bc of what it meant to them historically.
-
Racism kept many of us from giving our children the nourishment they needed from us. Let that wash over you.
-
We were forced to give milk produced for our own children to the children of our owners, forced to neglect the needs of our babies
-
Then we were blamed when our babies got sick or died and called “bad mothers”.
-
The connection btwn Black American women and breastfeeding has not always been positive and BF advocates have to know this.
-
So when I see WW, esp, coming down on BW for not breastfeeding, I cringe… it’s clear they’re not employing culture competence
-
I say barely half of Black women breastfeed, after several tweets talking about why (including historical violence) and then…
-
When BW were working and out of the home 16+ hours a day or barely allowed to go home to their children at all, how were they to nurse?
-
BW had few choices but to NOT breastfeed and supplement their babies’ diets with whatever was available.
-
And yet… BW have been perpetually vilified as being “bad mothers” when they’ve been forced into these conditions
-
@FeministaJones So would their relationships with their children, esp. from having to nurse & nurture White children at expense of their own
-
Re: #LRT, but BW were called “bad mothers”! Without acknowledging how much mother-child connection was sacrificed for work
-
Only in the last 20 years or so have we seen a significant cultural shift among Black women to nurse their own children, thankfully.
-
Because, real talk…? Sistas in the 50s, 60s, and 70s weren’t nursing, in large part bc they worked so hard and so long away from home.
-
And the stigma of BFing was “thats for them White babies”, which we can see how it came from resentment of forced nursing of White babies
-
@FeministaJones I see that as yet another form of economic violence. Formula isn’t free but we couldnt nurse cuz we had to work so much.
-
Let your mind wrap around one woman demanding that another woman take the milk she is producing for HER own baby and give it to hers
-
Breastfeeding, in the mid-late 20th century, was somewhat of a privilege for those who could afford to be around their babies
-
How can we demonize economically disadvantaged women for NOT breastfeeding at a time before pumping, packaging, etc?
-
That was passed down through generations and only in the last one, w/advances in BF support tools, are we seeing more BW embrace BFing
-
My mother and all of her sisters formula fed. No one breastfed. My mom asked “What formula you plan on using?”
-
Cultural competence means not assuming a new Black mom is automatically taking the “Duh of course I’m breastfeeding” approach
-
It means understanding that our historical connection to breastfeeding is one of oppression, violence, and denial of “womanhood”
-
“From 2000–2008, the percentage of women who initiated breastfeeding went up from 47.4% to 58.9% for blacks” http://www.cdc.gov/breastfeeding/resources/breastfeeding-trends.htm …
-
Like I said, this is a relatively new cultural shift and it’s important to unpack and respect the negative connections to BFing
-
@FeministaJones My aunt was a “wet nurse” in the 80s in the south. When people act like this stuff is archaic…it’s not.
-
@FeministaJones That’s why I am always so wary of white women organizing and educating BW on BFing. They gotta do the knowledge!
-
Not just for Black women, for Black men as well. So yeah… we gotta unpack this stuff.
-
#WomensHistoryMonth The story of the Negro Nurse (an oft-overlooked figure in American history) http://docsouth.unc.edu/fpn/negnurse/negnurse.html …
-
“It’s a small indignity [..] no white person at the South ever thinks of addressing any negro man or woman as Mr., or Mrs., or Miss”
-
” It is a favorite practice of young white sports about town–and they are not always young, either–to stop some colored nurse +
-
” inquire the name of the “sweet little baby,” talk baby talk to the child, fondle it, kiss it, make love to it, etc., etc.+
-
“and in nine of ten cases every such white man will wind up by making love to the colored nurse and seeking an appointment with her.”
-
So remember when I said that not standing up to defend Black women is a behavior learned and socialized into BM?
-
And how, historically, when Blk men stood up to defend Blk women, they faced violence, imprisonment, or death?
-
If every time you tried to defend a Black women, you were on the receiving end of violence, what might you do, eventually? Stop.
-
“If their fathers, brothers, or husbands seek to redress their wrongs the guiltless negroes will be severely punished, if not killed” Oh
-
When I hear “Black women ain’t worth it…” talk, at the end, I hear the unspoken laments abt the repercussion for making us “worth it”
-
It gets passed on… it’s self-preservation…it has to be unlearned
-
If we loop Black men into the BF discussion, we have to ask how many are supportive of BFing and the economic implications for them
-
We have to think about how maternity leave affects Blk families where the men are struggling to find work. That’s loss of wages…
-
And if women feel they have to hurry and get back to work, they might not opt for BFing if formula feeding is easier.
-
Reading the nurse narrative, I wouldn’t be surprised if BFing was a trigger for Blk men back then too, in light of the WM “advances”
-
I wonder if any BM discouraged BW from BFing bc it reminded them of maybe what their own moms went thru as wet nurses for WW
-
Hard to think of breastfeeding as violence against women, but for Black women in America, the history shows it has been.
-
!! RT @Alivada: @FeministaJones keeps periods at bay too …in an era pre bc …so if partner was wet nurse, couldn’t parent themselves
-
If BW were forced to keep lactating for wet nurse purposes, the impact on their own fertility/reproduction would likely be great.
-
So that’s my #WomensHistoryMonth chat for the weekend.





What About the: Respiratory Therapists?
Ready for a happy story?
Respiratory therapists are responsible for a lot of things all over the hospital. When they are on our floor, I can hear their phones ringing to call them to another floor. We see them doing treatments frequently, we call for help occasionally, and they are always included in a rapid response (a team effort to get to a deteriorating patient and avoid a code).
I am good with trachs, due to extensive training while I was a tech, and later homecare experience. So I am very comfortable with suctioning and trach care. Often, if the RT is very busy, I’ll do as much as possible to make their night smoother. I also volunteer to take the trach patients as often as I can because I know most of the nurses on my floor don’t like trachs. These patients often request for me to be their nurse again and again, and I do. It helps that I’m an excellent lip readers and intuitive. I rarely feel fear with a trach.. it’s a stable airway.
Recently at work, I felt helpless. It was a busy night, I had a 6 patient load with some really heavy patients. My patient was deteriorating and a call to the resident was fruitless. I suctioned, but it was like tar. It was bad. My patient was grey. The oxygen level was okay so far but could get worse at any moment.
For the next 1-1 1/2 hours, two incredibly knowledgeable RTs worked over my patient, performing procedures I’d never even heard of. They told me what medications to get from the doctor. I phoned and phoned and phoned. I brought the meds in. I medicated the patient for pain. Other respiratory therapists in the hospital started to pick up their work, but I know they got behind.
It’s the middle of the night in the hospital. We ran out of suction catheters. The house supervisor went to central supply and when she couldn’t find what we needed, so she called floor after floor and suction catheters start to appear. We were good.
I was so impressed by the variety of the things they could do, and within that hour to hour and a half, my patient began to breath better. Partially from pain medication, but mostly from sheer force of will. We are all very bonded to this patient and he to us.
I was also impressed by the nurses and CNAs who left their floors running with the equipment we so desperately needed.
When I left that morning, the patient put out a hand. Thanked me for all I did. I said
You’re welcome, but it was a team effort and you are the most valuable player in the team.”
A lot of times, you’ll have a bad shift and you’ll feel you didn’t give the best care, and you’ll say to the oncoming nurse “well, they’re all breathing.” It’s nurse code for “I could only do the bare minimum, but we all survived, can I go home now please?
That night, I learned more about what respiratory therapists do. Like nurses, they run hard, unlike nurses, they are spread throughout the hospital covering several floors at a time. I knew they were smart, good in a crisis, but I am so moved by gratitude.
When I left work, everyone was breathing. And that is because the respiratory therapists I work with put their feet down and said “no.” It was a rough night, but we gave excellent care. And honestly, I don’t begrudge that patient my break (I did manage to eat). In a perfect world, nurses could get breaks everyday but medicine is by its own nature an imperfect science, and while I complain if I don’t consistently get breaks, it is absolutely worth missing a break to improve your patient’s health.
I plan on writing a series of blog entries about my interactions with other medical professionals. As with my patients, I will not name names or identifying features. The only person’s privacy I am giving up is my own.
Update on – The Effects of Nursing on Nurses
I’m going to address a few things I read repeatedly in the comments of my original post:
What about the CNAs/PCTs/Aids/etc? I was a tech prior to becoming an RN, while I went through nursing school. I personally know how exhausting and backbreaking the job of a tech can be. But this post wasn’t about CNAs, it was specifically about nurses. CNAs do not have the same responsibilities nurses carry, although we share many of the same tasks. The RN is ultimately responsible for the task to be completed, and will be held responsible if it is not. I do recommend CNAs take time to practice self care and realize when they are overly stressed, or if a patient is being abusive . I have personally seen patients abuse a CNA who would not abuse a nurse. CNAs are not mindless automatons, they are living, breathing people with a lot of their own responsibilities, and deserve to be treated with respect by nurses, doctors, and patients. Ultimately, my blog post was about nursing, and because I was not dealing with a CNA at the time, CNAs were not mentioned in my post.
If I don’t like my job, I should quit it. Also, I should have known nursing was hard when I went into nursing school. – I’m not going to quit my job. I’m very good at my job. My blog post was about encouraging all nurses, including myself, to practice self care techniques to avoid the effects of compassion fatigue. For those who are unaware, compassion fatigue is not the same as burnout. Compassion fatigue is the result of repeated exposures to extreme stress over time. When units have high levels of compassion fatigue, they have higher incidents of falls, medication errors, and infections. Nurses suffering from compassion fatigue do not answer call lights and alarms as quickly. Compassion fatigue is a real issue among healthcare providers. The recommended treatment for compassion fatigue is time away from the source.
If every nurse who suffered from compassion fatigue, stress, frustration or burn out left nursing, healthcare as we know it would be irrevocably changed.
I’m a nurse. I’ve never called in sick, taken a mental health day, or complained about the long hours and working holidays.
Congratulations. Maybe you should write your own blog post about the stressors you experience on the job, and how you deal with them so the rest of us can learn. Maybe you are one of these nurses who practices lateral violence, and are part of the problem.
Other healthcare professions experience the same thing. Why weren’t we included in this post?
I’ve said it repeatedly in the comments: this post was about a specific interaction between nurses. Other healthcare professions certainly experience stress, compassion fatigue, and lateral violence. We all have a lot of responsibilities. I cannot write about problems experienced by respiratory therapists, paramedics, EMTs or other healthcare workers because I have only been a secretary, a tech, and a nurse. I write what I know. If you would like to write a blog entry about your specific profession, I would be happy to link to it on my blog.
Since last August, I have taken several steps to improve my personal stress level and mental and physical health. Because I am attending a BSN program that has clinicals, and am very fortunate to have a very supportive spouse, I have decreased my work hours for the next several months while I have nursing clinicals. This will also allow me an opportunity to help my feet heal, as the pain during work is quite significant. I realize not everyone can do this, and that I am very fortunate. I will still be spending 36+ hours a week on the hospital floor, as well as time in classes, so I will remain pretty busy.
I would like to recommend some reading for those interested in the problems facing nurses
From Silence to Voice: What Nurses Know and Must Communicate to the Public – Bernice Buresh and Suzanne Gordon
Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes and Medical Hubris Undermine Nurses and Patient Care – Suzanne Gordon
Good Morning
I have approved all pending comments. I will not be making any further comments on the “Effects on Nurses” blog for a couple of days.
I’m really overwhelmed by the amount of attention this post has gotten.
I’ve seen a lot of people tell me to just get another job, like it was easy to switch from being a nurse to being something else. You’re missing the point. The point is that hospitals, nurses, administrations, need to work together to avoid the dread many nurses feel before a shift. We need to ask, what is it about nursing that makes injury seem preferable than going to work.
For those of you unfamiliar with compassion fatigue, I suggest you look it up. It is different than burnout.
For everyone who has told me to get another job. I’m really good at my job. I like the majority of my coworkers. I like my boss. I love my hospital. Just because my job is physically and emotionally stressful doesn’t mean I want to leave it. With my post, I wanted to encourage nurses to support one another and to practice self care.
Going to sleep now. Have a nice day.
Bribery
It’s happened to nearly every nurse I know. You work your ass off for a patient, and at the end of the day, the patient or family member try to give you a large cash sum in thanks for your work. I’m not talking about a $5 gift card to Starbucks, I’m talking about a gift of over $50 cash, or of a great deal of worth.
I remember caring for a woman who had emergency surgery but also had Alzheimer’s. She was traumatized to be out of her nursing home. She refused to eat anything. I worked with her for 3 days, helping her walk, making sure she didn’t fall, bathing her, and ordering different foods until I found something she would eat. It involved calling the nursing home and finding out from their staff what her favorite foods were.
I became close to her family over this time. Her son repeatedly thanked me for all my work, which was really nice. He nearly cried when his mom started to eat a peanut butter and jelly sandwich, cut into perfect squares. Every morning when he arrived and saw her clean and cared for, he knew his mom was safe.
At the end of my third shift with this pleasantly confused and challenging patient, her son pulled me into a corner and tried to give me $100. “Take your husband out to dinner.” I politely refused, and told him his thanks was more than enough. He insisted he wanted to give me a gift, so I suggested he send the floor a fruit basket, something we could all share. He begged me to take the money, but I told him it wasn’t right, because caring for his mother was my job. He said I did more than my job, but nurses know, I may have gone a little bit above and beyond, but not far. I politely said no a third time, and told him to take his own wife out and relax now that his mother’s health crisis had passed. He finally agreed.
After the patient was discharged home, multiple fruit baskets arrived for night and day shift, for each side of our unit. Everyone was really happy about that.
Not taking money from patient family members is one of the basics of nursing ethics. It could be construed as a bribe to give one patient better care than another, which I just won’t do. You get care based on how much care you need, not how much care you can afford.
So imagine how I feel every time I hear about a politician taking bribes for things like hot tubs, home repairs, vacations, etc.
It makes me want to vomit. Consider Bob McDonnell, who has been accused of taking multiple bribes. He makes enough money. He didn’t need those things. If it comes out to be true, it’s going to be horrible.
I am always amazed at the frenetic energy the wealthy or well-to-do spend on BECOMING MORE WEALTHY. You already can support yourself in luxury. The governor gets free food! A mansion! After he’s done, he’ll have speaking opportunities, book opportunities, maybe a pension (I don’t know what happens to Virginia governors after they leave office). Before this bribery scandal, even becoming Vice President was a realistic option. Instead, he had to take money and services from people.
Shame on Bob McDonnell, and shame on every politician who takes bribes. I’m not even talking about funding for political campaigns, I’m talking about out and out bribes. Shame on you. I would never solicit bribes from a patient or family member, how dare you do this to your constituents, who look up to you.
Vanderbilt Hospital In Nashville Has Nurses Doing Housekeeping
NASHVILLE, TN (WSMV) –
Vanderbilt University Medical Center’s latest budget moves mean nurses will be responsible for a lot more than patient care.>
The Channel 4 I-Team has learned some Vanderbilt nurses will now be in charge of cleaning patients’ rooms, even bathrooms.
Sanitized environments in hospitals are critical to a patient’s health, but the new cost cutting measure has at least one nurse concerned.
“Cleaning the room after the case, including pulling your trash and mopping the floor, are all infection-prevention strategies. And it’s all nursing, and it’s all surgical tech. You may not believe that, but even Florence Nightingale knew that was true,” said a hospital administrator to staff in a video obtained by the Channel 4 I-Team.
The new cleaning changes were also detailed in an email sent to staff of the Vanderbilt Medical Center East team, which – according to a hospital employee – works in surgery areas and patient rooms.
A manager writes in the email, “We have undergone some major budgetary changes … this means we will need to pull together like never before.”
The email says nurses will now have to pull their own trash and linens, sweep up and spot mop. Nurses, care partners and nursing assistants will be responsible for all patient care areas.
“The priority will be what the patient sees,” the email states.
Also, in bold highlighted text, the email says, “Be sure to wear the appropriate [personal protective equipment] when doing any disinfecting – that includes, a cover up gown, gloves, mask and even an eye shield when necessary.”
Nurses were also told to “refrain from speaking negatively about this in an open forum where our customer can hear. If you need to vent come see me.”
The hospital employee did not want to be identified for fear of losing her job but wanted the public to be aware of the changes.
“This is our new reality. The work still must be done. We must still care for patients, and we must do so in an efficient manner,” the hospital administrator told staff in the video obtained by the Channel 4 I-Team.
The nurse to whom we spoke says before these changes, the hospital’s environmental services department was in charge of cleaning those patient areas and that staff does not have interaction with patients.
The nurse is concerned that doing both cleaning and patient care could lead to cross contamination.
The email obtained by the Channel 4 I-Team does say environmental services will still be handling some cleaning.
In a statement, Assistant Vice Chancellor John Howser, said:
“The safety of our patients is always of foremost concern. All decisions about operational process redesign at the Medical Center are being made in a patient-centric manner and will not affect the safety of patient care.”
The Tennessee Department of Health says it does not specify how a hospital chooses to clean, as long as the employees are appropriately trained and follow CDC guidelines.
If they do that, the state says there should not be any increased risk of infection.
We checked with Lipscomb’s nursing staff. The executive associate dean of nursing, who has been a nurse for 25 years, says she hasn’t heard of a hospital doing this before.
Copyright 2013 WSMV (Meredith Corporation). All rights reserved.
This really bothers me. As nurses, we already have hundreds of responsibilities, and I believe Vanderbilt’s choice to have nurses clean toilets and mop floors may lead to cross contamination as well as an increase in patient falls and medical errors. I am certain they are not going to decrease the nurse:patient ratio in order to make this change easier on the nurses. Vanderbilt is looking for ways to slash jobs, so they are getting rid of EVS because they can only legally get rid of so many nurses.
Especially insulting is the implication that Florence Nightingale would have wanted nurses to return to doing housekeeping in the hospital. Nightingale wanted nursing to move forward, not backward.
Please help me get this out on social media! Retweet, reblog. Post it on Facebook. Don’t let Vanderbilt harm patients and nurses this way! Use the #Vanderbilt hashtag.
The Effects of Nursing on Nurses
Hi, welcome to my blog post. I have never had a blog post get more than 50 comments, so I am a bit overwhelmed. After responding to many comments, here is a note:
Note: I wrote this blog entry at the end of my 3rd 12 hour shift in three days. I was tired and I was emotional. It is a blog post, not an “article.” It is not researched or sourced, it is purely opinion.
The point of this post is that nurses (and many other professions) need to take the time to practice self care and to encourage one another to practice self care.
My biggest mistake in this post (and there are many) was to use “her” or “she” when I should have used “they” or them.” I ignored my male coworkers, and I should not have. You have my apologies, and I have corrected the post. I have left “she” and “her” in place in the portion where I talk about my coworker.
I have read every comment posted and deleted some very nasty comments that were not helpful to conversation. If you feel this is the place to spew your vitriol, it is not.
August 11, 2013
This morning, while I was giving report to the day shift nurse taking over my patients, she burst into tears.
She’s going to miss her children’s hockey play offs due to our strictly enforced every other weekend schedules. You work every other weekend, no more, no less, unless you are going to college (I work every weekend because I’m in college). She’s their hockey coach, and inevitably, each year, their last game falls on a day their mother has to work. I’ve come in early for her before.
So I offered to come in on my night off for an hour and a half so she could get to the game. I’m coming in that early because I know she won’t be done charting.
She turned me down until another day RN got involved. I reminded my coworker I only live a mile from the hospital, and it really wasn’t a big sacrifice for me. She finally agreed, and calmed down. We got permission from the charge nurse.
Nursing is one of the largest professions in the world. If you don’t know a nurse, I’m really surprised. Nurses talk a lot about the rewards of nursing. Catching that vital sign, saving lives, providing comfort, but nurses, by nature, are taught to martyr themselves on the altar of nursing.
When I was a new grad, I hated coming to work so much that I would wish I’d get hit by a car on my way to work just to get out of work. One night, while checking medication sheets, I confessed this to some experienced nurses and found out some of them still felt the same way.
In nursing, it is NORMAL to have days where you wake up and just can’t mentally and emotionally face the day at work. I swear, the only other people who can understand this are nurses.
Nursing is emotionally, physically and mentally taxing, and some days you run too low on what you can give emotionally, physically and mentally. That minor back injury you don’t want to report to HR because you don’t want it on your record. Having a patient with constant diarrhea who can’t get out of bed and needs to be physically rolled and cleaned several times an hour. The cold you got from the two-year old someone brought in. The sorrow that comes from supporting someone who has just found out they were dying, holding in your own tears so you could wipe theirs. In one day, all of those patients could be yours.
I don’t know a nurse who hasn’t taken a mental health day. Some do it by requesting more vacation than others. Some do it by calling in sick, but it’s all time off because we are too drained to give anymore.
So if you know a nurse, and that nurse mentions to you that they feel like calling in because they just can’t take it another day, don’t give them a hard time. Especially if you have an 8-5 job with weekends off or some other really great schedule. The 12 hour shifts nurses work mean we miss the entire holiday we work with our families. Night shift nurses have to choose between holiday dinners or sleep. Often, if a nurse chooses to sleep rather than go to the holiday dinner, guilt ensues. Even though I’ve told my mother-in-law repeatedly that every nurse has to work holidays, she makes a point to say how horrible it is my husband has to be alone for a few hours. What about me? Working my ass off while everyone else celebrates?
We work hard. We are intentionally understaffed by our hospitals to improve profit, even if the hospital is a non-profit. We help people at the worst times of their lives, and often have no way to debrief, to get it off our chests. We don’t just bring warm blankets and pills. We are college educated, degreed professionals who are often treated like uneducated, lazy servants. We get sexually harassed by our patients. We get groped, punched, cut, I even know of a nurse on my floor being strangled (she survived).
Nursing can be rewarding. But nursing is a fucking hard job. If you are afraid of healthcare rationing, you should know it is already happening. Nurses are unable to give everyone the care they need, so patients with smaller problems may not get the same level of care. A nurse may be pressed to only give the minimum amount of care to a patient if they have 5 or more very sick patients. If you don’t want healthcare rationing, talk to your local hospitals about their nurse to patient ratios. Talk to your doctors. If you hear of legislation to support nurse to patient ratios, vote for it. Support it.
So if a nurse needs a day off, you support them. If you’re in a position to help like I was this morning, do so. If you are a nurse, go easier on yourself when you think about the things you didn’t finish, or the things you should have said. It’s a 24-hour a day job and you don’t have to do it alone.
As of January 27, 2014, this post is no longer accepting comments. I am doing this as a practice of self care. Tending to this blog post, several times a day, has become a burden. It has had over 2 million hits, and I am tired. The post has become a platform for people who want to propel their own agendas and are using my space to do so. Thanks to all who said such nice things, and to everyone else, go write your own blog.
A Nursing Post
On my first shift as a Registered Nurse, I went into a patient’s room to change her IV fluids. Instead of taking down the bag, I just pulled out the spike, showering myself in D5. The patient and my preceptor laughed so fucking hard.
A few years later, I was taking ice in to do a dermatome check, reached up to grab a glove to put it in, and poured ice down my scrubs in front of the patient and his 5 family members, who laughed their asses off.
For my last JoAnne moment of the day, someone spilled vanilla ice cream on the floor. I came running around the circular nurse’s station, I always move quickly, slipped on the ice cream, went airborne and fell on my ass. I got a standing ovation from the doctors, patients, and nurses, as well as a trip to the ER.
*bows*
